It's an emission light source or probe that can be directed to specific cells with targeting agents. On our website (www.bikanta.com) you can find links to some of our publications and if you would like more literature and information about nanodiamonds, we'd love to share with you. Email us at [email protected]
You are correct in the fact that the kidney's are one route of clearance for small agents that are injected. However, these are typically small molecule agents or particles on the lower size range at a couple nms in diameter. To reference a highly sited scientific article from Chemical Rev (Chem. Rev. 2010, 110, 2921–2959), "At 8 nm, observations have been made that hepatic uptake begins to dominate clearance routes, and by 10-12 nm the reticuloendothelial excretion route becomes the dominant route for clearance."
These nanodiamonds range in size from 15-100nm, so the kidneys will not be their primary route of clearance. It is also crucial to note that with any nanoparticle development, coating is a major factor in its biodistribution behavior. Coatings can and have been designed in more recent work regarding nanomedicine that minimize various biodistribution issues.
If they are in fact small enough to escape via biliary excretion, that would be great. But just skimming the literature it looks like they can accumulate and persist for weeks in the liver—a situation which would suggest hepatotoxicity is another problem (Zhu et al 2012 in "Theranostics" -- never heard of that journal but paper looks 'ok').
Coatings won't help this problem unless you can somehow change the shape of the crystal to fit through the slit OR get it to cross into the renal luminal space via transcytosis or excreted more efficiently in the biliary tree. All difficult propositions.
I really hope novel techniques like this work but this particular on seems very problematic. If I were you I would complete a serious set of toxicity studies very early on to make sure this isn't a fish that's dead in the water.
Toxicity concerns are always utmost to consider when developing tools for the clinic! Thus far, all studies regarding nanodiamonds have shown biocompatibility and non-toxicity. Coming from a research background and having done a number of in vivo studies myself, these studies we plan to repeat with each targeted version of the nanodiamond (particle + ligand such as antibody) before reaching the clinic. To clarify, we are at the pre-clinical level currently.
Hi everyone! I'm Ambika, one of the founders of Bikanta and inventors of this technology. I'd love to answer any questions that you may have. Here is also a link to our website: www.bikanta.com
Thanks for the share from PG's article. We are definite believers that it is possible to detect cancer significantly before symptoms begin to appear!
My general understanding in health startup world ("real" health startup - not just a new mobile app that measures vitals) is that if you have a truly compelling product that is clinically proven (sounds like this is?) then the venture/acquisition/funding landscape is pretty straight forward and has high returns - something that doesn't generally characterize the path of the AirBnB's, Heroku's, Homejoy's, etc. of the world.
I'm glad you asked! I would encourage you to look at this article where YC recently announced how it will be backing bitechs: http://www.nature.com/news/start-up-investor-bets-on-biotech.... We are excited to see this shift in attitude towards biotech investing and wanted to jump on board early. What makes us a a fit for this is our business strategy that is a closer fit to the "style" of companies that come through YC. For a typical biotech with clinical targets in mind, to bring those to market after FDA approval and clinical trials is a long process with returns being 7-12 years down the line. In our case, there is an identified research tools market that we can tap into first that would make us profitable by next year. By establishing an early source of revenue, we mitigate risk for our investors. Through YC we have a platform and the opportunity to reach wider umbrella of investors to share our story and strategy with.
I think anyone could answer this question -- fundraising is extremely time consuming, which means less time for actual product development. YC is the fundraising strategy since the demo day blasts lots of investors with the same chunk of information which is more efficient than individually pitching to each investor through typical fundraising processes. Investors are typically picky on who can pitch them, so unless you have an intro, it's hard to do a cold-call pitch. YC is a fast way to get an intro to everyone in the valley.
Howdy! I definitely understand your comment and the reason why I ask is bc typically biotech firms don't fit the early stage model, so I was just trying to get more info on why he chose the early stage model (past his stated reasons of not having a long time to market)
My thoughts exactly. Also, depending on the location, there are typically a large amount of public funds earmarked as grants for commercialization in this field. It's not the typical tech-company fundraising situation either. The marketing needs are also vastly different from the companies you mentioned.
We are planning to pursue the SBIR grant route, but there is a lag time in the grant application process and we are eager to supplement our current developmental traction in the meantime with funds from other sources as well.
In a long-ago materials startup, we had 30+ Phase I, 6 Phase II and 3 Phase III SBIRs. The money was helpful (VC funding on topic was thin at the time).
Very few of our SBIRs were exactly on point with our product development goals. This created resource allocation tensions around pushing product development vs. performing on the SBIR contracts. Something to consider when thinking about SBIR funding.
The issue I have is regarding how this technology will be applied to a population. If this is for screening, then it has to be incredibly safe and cheap. If this is for follow-up of known cancer, then you aren't going for 'early detection,' micromets, etc. as you suggest.
So assuming this is intended to be a screening tool, is there any feasibility data regarding fluorescence from even more than a couple centimeters within human tissue? I am skeptical that you will be able to see a lung or colon tumor for example... two of the three most common cancers in America.
I am a physician and consider myself very knowledgeable in imaging (Radiologist) as well as fairly informed about optical imaging (large institution with quantum dot and other types of opitcal research).
The in vivo pathologies and applications we are targeting initially are primarily nearer to the surface (i.e metastatic node detection, skin pathologies) or procedures where surgeons can use NIR fluorescence imaging systems that simultaneously display color video and NIR images have been developed for real-time surgical applications. Though this wasn't a focus in today's article, along with in vivo applications, we are working on a number of applications for microscopy and ex vivo diagnostics.
what exactly is the mechanism of bioaccumulation in cancer cells specifically? Or is this merely an imaging method that will have to be conjugated to, say a cancer-marker antibody?
This is the key issue. Detection by antibodies or some other label will be the true discovery. Binding that to nanodiamonds or whatever isn't the bottleneck.
Well we have plenty of biomarker candidates (aka human genome project) and, following them will come plenty of monoclonals, which should be relatively easy to humanize. The bottleneck may be 'bioinformatics', and I don't think bioinformatics is going to be a 'embarassingly parallelizable' problem, certainly not in the sense of "throw more people, computers, and bioinformaticians at the problem" sense.
Looking at some details on the technology, I would have to disagree. Nanodiamonds seem to be a much better fluorescent label than what is traditionally conjugated to antibodies. Traditional conjugated fluorophores have high susceptibility to bleaching, so you have to sort them out from natural signals. With nanodiamonds, it appears you can bleach all the natural signals and get a clear signal from the nanodiamond. This is pretty cool.
You missed the point. Detecting the protein or whatever that is deregulated in disease early is the hard part, not the fluorophore or nanoparticle to which it conjugates.
Are you concerned by the FDA's announcement that they intend to regulate lab-developed diagnostic tests in a similar manner to medical implants and devices?
Is the technology going to be affordable ?
I'm a big believer of free/affordable health care and such technology could have a big impact around the world.
I used to study nano and I remember hearing about nanodiamonds 3 years ago in the context of medical diagnostics. It's really exciting to see more nano stuff taking off as startups.
Major props for using a cheap source of nanodiamonds. Any issues getting ones that are the right size/shape?
Thanks for the props! We plan to offer a few different sizes of the brightest diamonds possible to our customers. The sizing and separation of the nanodiamonds can be accomplished a few different ways, the challenge is always in preventing aggregation. Bikanta's secret sauce is in our process to stabilize and functionalize the particles, irregardless of what the size and initial residues are on the surface.
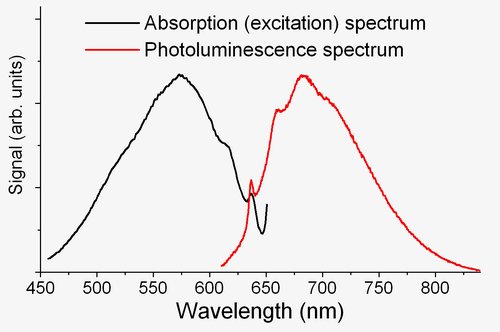
What's the fluorescence emission mechanism, defect sites in the crystal lattice? What's the QY? What's the absorption spectrum look like, especially in the NIR range? If we were exciting these particles at 785nm, what would the emission spectrum look like (peak and FWHM)? Is the YC startup focused on the nanocrystals themselves, or on imaging agents including a targeting ligand?
Sorry for the basic questions, I no longer have journal access :( and this sounds neat :)
I'm happy to answer these technical questions. It's nice to share that info as that is what makes them so valuable. The fluorescence comes from nitrogen-vacancy centers. Here is a link showing the excitation and emissions spectrum. http://upload.wikimedia.org/wikipedia/commons/8/85/NVple.JPG
The Stokes shift, as you can see is very large. The quantum yield is 1 and they don't blink. We are initially focusing on stabilized nanodiamonds with various chemical groups put on the surface to have them ready for further conjugation. Email us at [email protected] and I can have a further conversation with you if you would like.
For in vivo studies, and even possible human studies, have you given any thought for how you will do PK/BD on these? I'm having trouble imagining how you'll be able to detect these non-optically, unless you had some made of heavy isotopes for ICP/MS.
Continuing with the human studies thought, are these particles seeing RES uptake? I assume, based on the high QY, that these the emission centers for these particles are protected by a thick shell and/or corona. General handwaving from the FDA was that they were as concerned with particles persisting as with elemental toxicity. Is there a predicted degradation pathway for these particles?
Can these particles be made with a hydrodynamic radius, including corona, <8nm? Is it possible to dope them to get better NIR emission?
Unrelated to technical stuff: I thought that a YC thing was that you had to move to San Diego for a few months. That doesn't seem all that conducive to wet lab work, in fact, it seems like a non-starter. Is that still a requirement for the bio-related startups? If so, how how disruptive is it?
these probes can be visualized by standard fluorescence imaing instruments including fluorescence microscopes, TIRF, gel scanners, flow cytometry, optical animal scanners, clinical cameras etc. They also have long fluorescence lifetimes and so can be imaged by fluorescence lifetime instruments. What the article didn't delve into is that because of an additional magnetic sensitivity that the nanodiamonds have, we can improve image quality and imaging deeper into tissue with an additional hardware piece that we can add on to existing systems or in a stand-alone system that is cheaper to be tailored to n=only nanodiamonds. if you want more info on this, I can elaborate or have a chat with you
PSA tests are very controversial because many believe early detection of prostate cancer leads to worse health outcomes as many men get surgeries to remove cancers that will have no material impact on their life expectancy or quality of life.
How do you plan to deal with the fact that early cancer screening may be detrimental to health outcomes?
Sorry to ask late, as I thought this would be first question: how does this work? That is, how do the nanodiamonds get into the body, and how are they flushed afterwards? I like the idea but the article seemed rather thin on details of how this would operate in practice.
{kind=link}