As it happens, I currently have COVID. When I first noticed I was getting sick, I was scheduled to fly in the near future, so I got a rapid COVID test that delivers results in 15 minutes.
It was negative. I got another one, and it was negative too. I had thus intended to go ahead with the trip under the assumption I had a minor cold.
Later, a few days before I was to fly, I lost all smell and taste. Now I didn’t know what to think. I wasn’t particularly congested, and the loss of smell was total. I’d never experienced this before. Could both tests have been false negatives?
I delayed the flight (free of charge luckily, so no big deal) and got a test that had to be sent to a lab for analysis. A week later, the positive test result came back.
Take from this what you will. I'm not a scientist or a doctor and frankly there's nothing remotely intelligent I can say about the various tests out there for COVID. But if the rapid tests are as unreliable in general as they were for me, it’s sort of no wonder COVID is spreading like wildfire. I was very, very close to boarding a plane with an active case of COVID, and I would have if I hadn’t acted out of an abundance of caution.
Rapid tests are known to be unreliable and particularly have a high false negative rate. That's why all the guidance has been that rapid tests can be used to indicate infection but not rule one out, and none of the screening processes based on exposure and symptoms accept “but I also had a negative rapid test” as neutralizing a flag on any screening factor.
> I would have if I hadn’t acted out of an abundance of caution.
The bare minimum of caution with a rapid test is treating a positive as a true positive and a negative as an indicator that you need a regular test. That you understood your actions to be an abundance of caution demonstrates a failure to effectively communicate on some level (I'm not saying that you are culpable; the information is out there's but delivery is...mixed, even before considering how it is muddled by misinformation from various sources.)
I definitely think there's a communication deficiency or breakdown happening, because none of the medical professionals indicated to me that the rapid tests were that unreliable when it comes to producing false negatives. I also feel personally guilty for not having been as well-informed as I should have been. I'm just glad I experienced a tell-tale symptom (loss of smell/taste) and was able to act on it before boarding a plane.
Another interesting aspect of this is that prior to experiencing loss of smell/taste, I was more or less told by urgent care staff that I didn't have COVID, and they were pretty resistant to testing me -- hence I only got rapid tests. Yet I actually was right in the midst of an active case.
> Are they just flat out missing some infections, or do they require a much higher viral load to indicate positive?
they do require a higher viral load than the pcr test to accurately show infection. the pcr test studies have shown to be 0-30% false negative later in the illness after symptoms have shown (when there are fewer antigens in the body). both the pcr and the rapid tests are expected to have a near 0% false positive rate though with most false positives being lab contamination or mishandling. even if the test is 50% false negative(not the actual number) it would still drastically slow the spread of the virus coupled with other measures. This is more of a defense in depth instead of a firewall; the swiss cheese layers of threat reduction.
That's true, but in this case the converse statement is also true that someone with a positive rapid test should start isolating even if symptoms are absent. It's this latter statement that you were replying to.
> because none of the medical professionals indicated to me that the rapid tests were that unreliable when it comes to producing false negatives.
You're being very emphatic about this, but all you've described is that the rapid test failed in a single case (you). We expect a lot more failure than that from the slow test! Where is the idea coming from that you experienced egregious unreliability?
Well, he did take two rapid tests, which both produced false negatives.
What this tells us about false negatives depends on details he didn't mention, about how correlated the two tests were. Obviously, it was the same person each time - but was it the same day? Same test brand? Same clinic? Same tester?
I've had 2 nasal swab tests. The first one seemed to have taken a core sample of my eyeball or brain; the second one was not as bad. I have no idea if these were rapid tests or googles PCR tests. Messaging is poor for sure.
I can't count the number of communication breakdowns any more with Covid. Apparently to get any number of people on the same page about something is not possible. Even with the internet. Blame it on information overload, or perhaps apathy.
I hope when Biden takes office he does daily Covid briefings where they disseminate accurate knowledge which would include correcting previous things we thought we knew. I know democrats that actually watched the Trump briefings because there were actually intelligent people behind half the info. I think many people tuned out the moment he recommended injecting bleach - but there was still value in the briefings. It was something that I know a LOT of people actually paid attention to.
> I think many people tuned out the moment he recommended injecting bleach - but there was still value in the briefings. It was something that I know a LOT of people actually paid attention to.
This is an interesting comment re:communications and the messaging that reaches people. Trump did not recommend injecting bleach. He went on a rambling mostly incoherent recollection of a conversation he had where he was trying to learn what was being done. He was trying to sound smart.
His comments were all questions to the med experts. "Is there a way we can do something like that?" "Are we going to check on that?"
Yet everyone jumped on it saying he "claims" or "recommended". And it became "truth" because news articles covering the press conference used phrases like "claims" and "recommended".
> "So I asked Bill a question some of you are thinking of if you're into that world, which I find to be pretty interesting. So, supposing we hit the body with a tremendous, whether its ultraviolet or just very powerful light, and I think you said, that hasn't been checked but you're gonna test it. And then I said, supposing it brought the light inside the body, which you can either do either through the skin or some other way, and I think you said you're gonna test that too, sounds interesting. And I then I see the disinfectant, where it knocks it out in one minute, and is there a way you can do something like that by injection inside, or almost a cleaning? Because you see it (COVID19) gets in the lungs, and it does a tremendous number on the lungs. So it'd be interesting to check that. So you're going to have to use medical doctors, but it sounds interesting to me, so we'll see. But the whole concept of the light, the way it goes in one minute, that's pretty powerful."
Presumably, Trump had been briefed about all of these things before giving the "inject bleach" press conference. The press conference is not the time to be asking questions you just thought about of medical experts. Not if you are the one giving the press conference at least. That is where the messaging fell apart.
Especially with the internet. In the 80s the main media outlets reported the page and almost everyone followed. The internet now has a million “experts” for every actual expert, and even good opinions can doffer depending how you look at the facts.
I'm glad the OP made the correct decision in this case and hope they get well soon.
> the assumption I had a minor cold
> the loss of smell was total
Since there does seem to be a messaging problem about the reliability of testing, I think it's worth emphasizing: if someone has symptoms of COVID, they should proceed as-if they have COVID. CDC guidance[1] is to isolate if you have a positive test OR if you have symptoms.
To do otherwise is to gamble with the health and lives of the people they meet, and the people those people meet, and so on. It may prove almost impossible to show who caught COVID from whom, but that doesn't mean that ignoring guidance won't lead to deaths. A statistical death is still the death of a real person, even if we can't put a name to them.
To be clear, the order of events was such that I did not have loss of smell/taste at the time of the rapid tests. There was no indication at that time of anything that wasn't completely consistent with and expected from a cold, and I even encountered resistance when I tried to get tested prior to the tell-tale loss-of-smell symptom appearing (hence the rapid tests only at that point). I had a mildly uncomfortable phone call with an urgent care center where they discouraged me from pursuing testing because they didn't think I had enough symptoms.
I knew exactly from whom I had contracted whatever illness I had, and that person had also tested negative for COVID (upon further questioning, their test had also been a rapid one, and they too had not been informed of its unreliability for any negative determination).
> There was no indication at that time of anything that wasn't completely consistent with and expected from a cold
Unfortunately, I think these days symptoms of "just a cold" are enough reason to self isolate for long enough to reliably get through the Covid incubation period - which locally (Sydney .au) has been reported to occasionally be as long as 10 days or more.
The USA currently has nine million active cases. I actually think at this point if you have cold symptoms it may be more likely you have covid than a common cold.
(Though maybe someone has data in cold cases to clarify the cross over point)
> The USA currently has nine million active cases. I actually think at this point if you have cold symptoms it may be more likely you have covid than a common cold.
Your intuition is wildly off-base here. Nearly all of us catch at least one cold a year, mostly during the winter months. There are, quite literally, hundreds of millions of colds a year. There's also ~half a dozen viruses in circulation at any given time that cause cold-like symptoms, vs. one for SARS-CoV2.
The steps we are taking to reduce COVID spread also reduce the spread of the cold. I would be absolutely shocked if we don't end up having our lowest impact cold and flu season in decades this year. That isn't to say the grandparent comment is correct, just that you can't really use a comparison from prior years as an indication of how many people will get a cold this year.
In the first 6 months of 2020, Australian influenza deaths were down over 90%, attributed to Covid anti measures - mostly increased hand washing/sanitising, social distancing, and school closures.
If we assume that's representative of a 90% reduction in flu and cold cases (not guaranteed, but probably a reasonable estimate to reason about), then perhaps instead of "hundreds of millions" of cases, it might be down to "tens of millions of cases" of cold/flu. So maybe 9 million Covid cases means any cold/flu symptoms are somewhere between 50% and 10% likely to be Covid - a virus currently killing ~1% of the people it infects.
I am certain the prudent thing to do in 2021 is assume _any_ cold/flu symptoms are likely to be a virus that's quite capable of killing you (and/or the people around you) and act accordingly until you are 100% certain it's not. (Which probably means 2 negative PCR tests ~10 days apart.)
> The steps we are taking to reduce COVID spread also reduce the spread of the cold.
...and cases are going up, so it's probably safe to assume that there are lots of colds being transmitted, as well. And as I said, there are many cold viruses in circulation, at all times.
Even if you believe that "the steps we are taking" are working, you have to assume that they're disproportionately effective for the common cold in order to make the statement the OP was making. Say what you will about SARS-CoV2, but it's more-or-less like any other respiratory virus in terms of transmission characteristics. There's no particular reason to believe that anything we're doing would stop rhinovirus or RSV, but not SARS-CoV2.
This doesn't follow at all because you are comparing the current state of laxing COVID precautions to the previous state of near zero cold precautions. For example, tens of millions of people are currently working from home and the workplace is one of the primary places colds spread. If we treated COVID like the cold we would already be on the other side of the pandemic because it would have already ripped through the population and millions would be dead.
> This doesn't follow at all because you are comparing the current state of laxing COVID precautions to the previous state of near zero cold precautions.
I am not. There are, right now, 5-6 cold viruses in common circulation. There is one SARS-CoV2 virus.
Nothing we are doing would be expected to suppress other respiratory viruses, but not this one.
>I am not. There are, right now, 5-6 cold viruses in common circulation. There is one SARS-CoV2 virus.
Yes you were. In your first comment you said "Nearly all of us catch at least one cold a year, mostly during the winter months. There are, quite literally, hundreds of millions of colds a year." Those are numbers in a normal cold year. This isn't a normal cold year.
>Nothing we are doing would be expected to suppress other respiratory viruses, but not this one.
I'm not sure where this line of argument came from as no one was arguing against it. The assumption is that these COVID precautions are equally effective against the cold, flu, COVID, and other similar respiratory diseases. This will lead to a huge drop in those non-COVID diseases as the precautions we are taking are so drastic compared to a normal year.
> Yes you were. In your first comment you said "Nearly all of us catch at least one cold a year, mostly during the winter months. There are, quite literally, hundreds of millions of colds a year." Those are numbers in a normal cold year. This isn't a normal cold year.
You can divide the number by any factor you want, but there are still ~6x the number of viruses out there causing colds. Even now.
>there are still ~6x the number of viruses out there causing colds
The variety of viruses is totally irrelevant to the original question of what are one's odds of having COVID based on having cold symptoms. The only piece of information that matters for that are the aggregate numbers and aggregate numbers from previous years are misleading.
> The variety of viruses is totally irrelevant to the original question of what are one's odds of having COVID based on having cold symptoms.
It is an essential factor, unless you make the (implausible) assumption that we have essentially eliminated all other respiratory viruses except for SARS-CoV2.
I like how you cutoff the my quote at the exact point that shows you how you are wrong. As I said "The only piece of information that matters for that are the aggregate numbers".
Whether there is 1 version, 6 different versions, or 1 million different versions of colds is irrelevant to your odds of having COVID when you show symptoms. What matters is whether there is 1 person, 6 people, or 1 million people with colds. The variety is meaningless. What matters is the aggregate number of cases.
> The variety of viruses is totally irrelevant to the original question of what are one's odds of having COVID based on having cold symptoms. The only piece of information that matters for that are the aggregate numbers and aggregate numbers from previous years are misleading.
It is an essential factor, unless you make the (implausible) assumption that we have essentially eliminated all other respiratory viruses except for SARS-CoV2.
I catch colds roughly 7-8 times per year. It sometimes feels like I have cold symptoms more days than I don’t. I currently have cold symptoms. If I had to isolate every day I had a cough, sore throat, congestion, or sneezing, I’d be under house arrest most of the year. I think it’s vitally important that we have accurate COVID tests that can definitively distinguish a case of the cold from a case of COVID.
At the end of the day everything is a judgement call. In this case I believe you're an outlier, guidelines are usually structured for the general case. Should you specifically treat every cold like it could be COVID? Maybe not, but should somebody else who gets sick only 1-3 times a year treat every cold like it could be COVID? That seems a lot more reasonable.
Not to mention it is wise and courteous to stay home and avoid exposing yourself to lots of people when you are sick regardless of if its COVID or not.
Not everyone can afford to stay home with minor illness. Not everyone will be employed if they stay home and can't "cover" their days off with measly 40 hrs a year of paid time for such purpose ( if they have any paid time at all).
This issue existed long before COVID. COVID is spreading partially due to this issue. Many people have no choice but work to avoid homelessness and/or hunger.
You should be tested for primary immune deficiency, based on the frequency of your colds alone. If you do have primary immunodeficiency, it is treatable with subcutaneous immunoglobulin, in most cases. Either way, it is treatable.
I am personally on subcutaneous immunoglobulin for two rare immune-mediated neurological diseases, and I have not had a cold in over 3 years, when I would get them a couple of times per year. It helps tremendously.
These are the 10 warning signs of primary immune deficiency in adults:
Adults
If you have two or more of these signs, speak to your doctor about a possible Primary Immunodeficiency.
1. Two or more new ear infections within 1 year
2. Two or more new sinus infections within 1 year, in the absence of allergy
For the broader point, regardless whether or not someone is more likely to have a common cold or COVID given the same group of symptoms, I think the point stands that if someone has symptoms consistent with COVID they should proceed as-if they have COVID -- especially given the current case rate in US.
Are you sure? Do nearly all of us catch a cold _this_ year? I know the flu is way down this year due to covid-related behavioral changes. I'd be surprised if common colds are unaffected.
I agree with you, and that's largely why I wanted to share my story -- to illustrate that even without any tell-tale symptoms and multiple negative test results, you can easily still have COVID.
Thanks for sharing your story, it's useful to hear anecdotes. I also want to emphasize I was making a general comment and not intending a personal criticism.
The points raised by bigiain and mxcrossb are well-made, "cold-like" symptoms are COVID symptoms, the loss of taste and smell only occurs in some cases. CDC has a full list of coronavirus symptoms[1].
I fear that many are flying, socializing etc. when they are actually symptomatic (e.g. headache, sore throat) because they consider these minor symptoms, or perhaps they can just "hope for the best", but the severity of the symptom doesn't change whether or not someone is symptomatic.
The heck is the point of a test if not to confirm or rule out covid? He took two tests, came back negative and assumed his "cold or covid" symptoms were cold until he had reason to believe they were covid. Other than the tests sucking everything in the fact pattern is perfectly reasonable.
Any test has a certain percentage of false positives and false negatives -- in fact, you can likely tune your ratio of false positives to false negatives depending on what your priority is. On a community level, the statistics from testing are essential for monitoring the spread of a disease, but on an individual level a test can still give an incorrect result, so shouldn't be the only factor when making decisions.
For an individual, if they have a negative test AND no symptoms AND no contacts with known COVID-positive individuals, then they can proceed as-if they don't have COVID and take standard precautions. However, if they do have symptoms, then that might mean further testing is required.
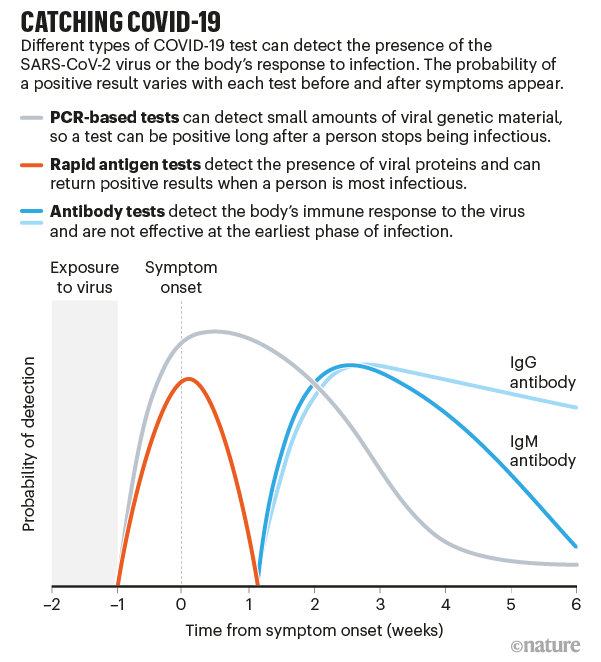
For anyone interested about testing, this graphic is essential:
It shows the difference in test efficacy for different tests (rapid antigen, PCR, antibody tests) as a function of time from symptom onset.
Rapid antigen tests only have a narrow window of efficacy. If they come back positive, you likely have COVID, but if they come back negative you could still have COVID and could still be contagious.
This is also why many countries are requiring PCR tests prior to entry, because they are more effective than rapid antigen tests, although can also give false negatives, especially early after exposure.
In my opinion, the rapid test's greatest value is using it to screen asymptomatic people in a regular (daily or weekly) process. For example, a school would test a random sample of students each day. This could help catch any stealthy clusters. It's not perfect, but it's better than just looking for symptoms.
It's also subtle in that while false negatives are common, false positives are rare (very rare). But general public don't get that subtlty and assume "the test isn't reliable" so a positive means they're not infected.
Almost no tests in existence can confirm or deny particular infection.
Think of them (and symptoms) more as odds updater. If you have 20 minutes to spare this video [0] by 3 Blue 1 Brown is a brilliant introduction to the concept.
Whether a test is positive or not depends highly on what type of test it is, and when you are tested relative to symptom onset. You can absolutely be carrying the COVID virus but still test negative. Heres a paper with a handy chart: https://jamanetwork.com/journals/jama/fullarticle/2765837
I think you testing negative was a combination of the rapid test being unreliable, as well as getting tested early with respect to symptoms.
Thanks for your anecdote. When SF was doing better and the possibility of big outdoor events with testing on the door were something that was being discussed, I looked at rapid tests together with some friends and the accuracy is really appalling. People relying on this to "safety socialize" may be one of the issues making cases rise in California, the math adds up. Many people reached to the government saying they should stop sponsoring and advertising rapid test sites because the false sense of security may be really doing more harm than good.
One of the rapid tests that we considered has, as advertised by its own manufacturer, a 10% false positive rate on basically all the population, and a 50% false negative rate even on symptomatic individuals with high viral load. Do the math, but using that type of test in something like for example a 100 person event or a restaurant will result in people being turned out of the door daily even if they were not symptomatic, and at least one or two people with high viral load being admitted into your place. I can't find the link of the test now, but there's better data about how harmful rapid tests are when not used together with PCR testing, for example here: https://www.bmj.com/content/371/bmj.m4941 and here: https://asm.org/Articles/2020/November/SARS-CoV-2-Testing-Se...
That's why most countries that really thought this through require a recent PCR test result for admittance.
It's really not clear what benefits rapid tests have if you don't have a model for population behavior. I think at lest the SF government is only doing them to save face now that the cat is out of the bag.
> But if the rapid tests are as unreliable in general as they were for me, it’s sort of no wonder COVID is spreading like wildfire.
Many rapid tests are indeed not accurate[1] but they still serve a purpose, depending on the sensitivity and specificity of the tests[2].
For the rapid tests with high sensitivity and you get a positive result, it's highly likely you have COVID.
For the rapid tests with high specificity and you get a negative result, it's highly likely that you don't have COVID.
And the public health measures of testing / contact tracing ONLY works if testing results come back quick. PCR tests are neither fast nor cheap, so those are not as effective in prevention of spreading because you don't do those all the time (slow + expensive).
I only have data points for two different testing orgs, but in my area, GoHealth charges $250 for a rapid test, and Color charges $110 for a PCR test[0]. So it seems like that's flipped from what you're suggesting?
The Color tests can even come back in 8 hours or so, if you're not too far from a lab and the lab isn't overloaded. Not as fast as 15 minutes, and certainly higher variance, but much more useful than 72 hours people normally assume.
Regarding false negative rate, Hawaii is accepting some of the rapid tests (like the aforementioned GoHealth test) for pre-travel screening, which is concerning.
[0] These are both without involving insurance at all. It's possible, though, that the Color tests are partially subsidised by Google?
This rapid tests have a very high false negative rate. The result you get back should really be "You have COVID" or "You may have COVID, get a PCR test".
Most countries which require a test for entry stipulate it must be a PCR test rather than a rapid (antigen) test. I’m currently in Lisbon waiting for the results of a 24h PCR test in order to board a flight to Azores, for example.
Rapid tests are at their most accurate when someone is at their peak infectiousness. Accuracy declines swiftly before or after that.
So the use you made of them didn’t fit their ideal use case, as you used them several days before travel.
Even then, with symptoms, I am not sure they would be enough to rule out a positive. The biggest use of rapid tests is finding additional positives that would not otherwise have been found.
> A week later, the positive test result came back
Which country do you live in that it takes a week for the PCR test to come back? It's around 24 hours here and I thought that was the case in all developed countries.
I'm in the US. The test was taken on a Sunday evening at about 7:30PM, and the results were delivered via text message the morning of the following Friday.
My guess is there's a lot of variability in how long it takes to get results. I know folks who've taken the same test and they got results back within 48 hours.
There's a lot of variability, and it depends on how far you are from the lab the particular test center uses, how quickly the test center sends your sample to the lab, and how busy the lab is.
I've had two tests that came back in around 48 hours and one that only took 8 hours (US, SF bay area). 4.5 days seems pretty excessive (and frankly pretty useless) though!
They've been using these lateral flow tests in the UK quite a bit - particularly for university students returning home/to campus (or at least, that was the plan!).
There is enough knowledge out there about the various kinds of tests (PCR, antibody, antigene) and what they're good for and what they're not. It's perfectly understood that while rapid tests are, well, rapid, they're much less precise than PCR testing. However, they are often better than nothing (you can't give a PCR test to everyone who wants to visit relatives in a nursing home), so they serve to minimise risk, not to remove it. (They also have a tendency to be more likely to be positive while you're actually infectious, which is not the same thing as having symptoms.)
I really don't think we should be discussing personal anecdotes during a health crisis, when there's enough data around that we can actually look at.
You were probably not contagious during those first days (at least for everyone except your partner).The threshold for the rapid test is higher than what the PCR detects. The antigen test is highly reliable for catching contagiousness, not just any viral load. Michael Mina (Harvard Biologist) presents the data in a great way if you want to check.
There are many different rapid tests. Some are reliable and some are unreliable.
For the ones that are reliable (like Abbott's test), they are highly accurate at determining whether someone is currently infectious. So you could have been infected but not capable of transmitting to others yet. These tests would be highly useful for onsite testing, such as if airlines required a rapid test right at the airport.
The most common error with these tests is false application. Did you have someone else doing the swab? It has to feel like someone is poking at your brain.
Sure, I'm in my early 30s. I do believe I had a pretty mild case all things considered, and I'm pretty much fully recovered at this point but still plan to quarantine for another week.
What I experienced was basically indistinguishable from a mild cold except for the loss of smell and taste, which took over a week to show up after the onset of the initial symptom (a fever). While I know loss of smell can happen from non-COVID infections, I can say this is the only time in my life I've had a total loss of all smell and taste. I'm very fortunate that this total loss only persisted for a few days, and at this point based on my subjective experience my smell and taste senses appear to be normal again.
If you still have yet to test positive for COVID you may not have COVID. A loss of sense of smell and taste is a common symptom of a viral infection.˜ [1]
Yeah - so you should probably go to a political rally or concert or a nightclub or something!!!
:sigh:
This is awful advice for 2021. (Even though _technically_ it's correct.)
If you have a loss of smell/taste you should 100% assume you have Covid and act accordingly, get tested immediately, self quarantine for probably 14 whole days, and get retested at around 10 days.
If you have "mild cold/flu symptoms" you should assume you like;y have covid, and should get tested (not with a "rapid test") and self isolate until you get a negative result.
Truth is, even with no symptoms, you could have Covid. If you've been in contact with anyone who has cold/flu symptoms, or been to a place where someone with a positive covid test has been - you should get tested (and probably self isolate until you get a negative result).
Results: The baseline assumptions for the model were that peak infectiousness occurred at the median of symptom onset and that 30% of individuals with infection never develop symptoms and are 75% as infectious as those who do develop symptoms. Combined, these baseline assumptions imply that persons with infection who never develop symptoms may account for approximately 24% of all transmission. In this base case, 59% of all transmission came from asymptomatic transmission, comprising 35% from presymptomatic individuals and 24% from individuals who never develop symptoms. Under a broad range of values for each of these assumptions, at least 50% of new SARS-CoV-2 infections was estimated to have originated from exposure to individuals with infection but without symptoms.
Conclusions and Relevance: In this decision analytical model of multiple scenarios of proportions of asymptomatic individuals with COVID-19 and infectious periods, transmission from asymptomatic individuals was estimated to account for more than half of all transmissions. In addition to identification and isolation of persons with symptomatic COVID-19, effective control of spread will require reducing the risk of transmission from people with infection who do not have symptoms. These findings suggest that measures such as wearing masks, hand hygiene, social distancing, and strategic testing of people who are not ill will be foundational to slowing the spread of COVID-19 until safe and effective vaccines are available and widely used.
> Yeah - so you should probably go to a political rally or concert or a nightclub or something!!!
I don't recall saying that.
> If you have a loss of smell/taste you should 100% assume you have Covid and act accordingly, get tested immediately, self quarantine for probably 14 whole days, and get retested at around 10 days.
Did I say otherwise?
What I said was, if you lose your sense of smell and taste and then proceed to test negative twice for COVID, you may well not have COVID.
Rapid tests are right 80% of the time. Two rapid tests back to back are right 96% of the time. That means after 2 tests there's a 96% chance you don't have COVID, and a 4% chance you do. That doesn't mean you should tour your nearest retirement community.
You shouldn't go out anywhere if you're sick in the first place.
[edit] Even then, there's a 1% false positive rate on PCR, and a 4% false negative rate on 2x rapid test. Even at this point there's a 20% chance OP doesn't have COVID.
> Rapid tests are right 80% of the time. Two rapid tests back to back are right 96% of the time.
I doubt the false negative % for two tests on the same person at roughly the same time are uncorrelated. (For two reasons: It seems logical that they would depend on viral load, and/or other non-random factors; And if they were independent, we would be able to achieve arbitrarily high specificity by taking and processing multiple samples -- just three would get you >99% -- which doesn't seem to be happening.) So the false negative rate for two tests might be much closer to 20% than 4%.
> That means after 2 tests there's a 96% chance you don't have COVID, and a 4% chance you do.
This part is definitely not accurate. The real probability will depend on base rates and facts about the individual case.
{kind=link}
As it happens, I currently have COVID. When I first noticed I was getting sick, I was scheduled to fly in the near future, so I got a rapid COVID test that delivers results in 15 minutes.
It was negative. I got another one, and it was negative too. I had thus intended to go ahead with the trip under the assumption I had a minor cold.
Later, a few days before I was to fly, I lost all smell and taste. Now I didn’t know what to think. I wasn’t particularly congested, and the loss of smell was total. I’d never experienced this before. Could both tests have been false negatives?
I delayed the flight (free of charge luckily, so no big deal) and got a test that had to be sent to a lab for analysis. A week later, the positive test result came back.
Take from this what you will. I'm not a scientist or a doctor and frankly there's nothing remotely intelligent I can say about the various tests out there for COVID. But if the rapid tests are as unreliable in general as they were for me, it’s sort of no wonder COVID is spreading like wildfire. I was very, very close to boarding a plane with an active case of COVID, and I would have if I hadn’t acted out of an abundance of caution.